By Bianca Lascano, PharmD, PGY2 Ambulatory Care Pharmacy Practice Resident, University of Mississippi School of Pharmacy
As healthcare professionals, we understand that social determinants of health have profound effects on health outcomes. Awareness of the health disparities they generate underscores the significance of emphasizing social justice principles in health professions education. It is important that educators help students develop the critical thinking, collaboration, and self-reflection skills necessary to foster a better society.1 There are several courses embedded in the curriculum that must be taught as students matriculate through the didactic portion of their professional degree program. There are many opportunities to discuss social determinants of health throughout the curriculum and help students understand their implications through the lens of social justice.
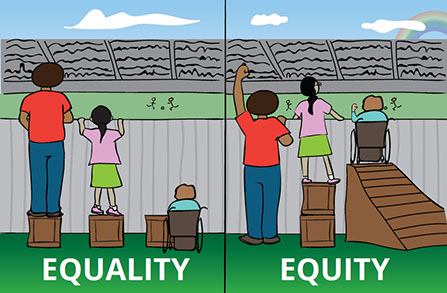 |
| Image from: https://www.promotionswest.com/health---social-equity.html |
In A Practical Strategy for Infusing Multicultural Content into Any Lesson posted on the Faculty Focus website, Dr. St Germain discusses a method to integrate multicultural content into each lesson he teaches in a business communications course. Dr. St. Germain gives specific directions to guide his students to think about marginalized groups. For example, if students are developing a website for the city’s recreation department, the directions would state, “evaluate how well the website ensures people of color and how welcoming the content may be to the LGBTQ community.” Having students work at the evaluation level of Bloom’s taxonomy, greatly increases the chances that the activity will allow the students to construct new knowledge as it pertains to cultural competence and social justice.2
Professors in the health professions can emulate Dr. St. Germain by including diverse patient populations when designing patient cases within each clinical module. Including social aspects of a patient’s life that might impact health outcomes and having students explore how that could affect treatment and healthcare delivery will prompt students to create individualized plans through the lens that is different than their own. Thus social justice issues can be woven into course material that, on the surface, appears unrelated to social justice.
It is surprising that even though issues related to social justice are central to healthcare services provided to patients, they have received inadequate scholarly attention. A lot of the course material taught within the health professions curriculum can be viewed from a social justice perspective. For example, we understand the treatment of hypertension can adversely affect certain patient populations more than others. Access to treatment and follow up care is more difficult for some populations. Food insecurity and lack of transportation can be significant barriers. It is important that students begin to recognize their assumptions and implicit biases as they explore and discuss case studies.
Unfortunately, implicit bias, by definition, influences health professionals without their knowledge and despite their best intentions.4 A process described as implicit bias recognition and management (IBRM) is required to mitigate the negative impact of bias. Research on IBRM suggests that as health professionals begin to accept that they can never eliminate all their biases, they also confront that they are learning within an environment that reinforces and contributes to these biases.5 Even well-intentioned learners may find the process of discussing and reflecting on biases challenging. Moreover, faculty may be reticent to facilitate such discussions.4
Sukhera, Watling, and Gonzalez propose transformative learning theory (TLT) as a guide for implementing implicit bias training in health professions education. TLT suggests that learning is a process triggered by disruption, followed by a revised interpretation of experiences that guide an individual’s actions.4 The process requires critical reflection, dialogue, and action. An illustrative example would be placing a health professional learner in a challenging rural or remote setting for service learning. This would facilitate cross-cultural interactions that produce dissonance, promote skill development, and require dialogue.4 This most certainly would be more transformative than a lecture about diabetes. Professors can assess engagement in these activities by inviting students to reflect on how their actions perpetuate the status quo. The goals of transformative learning are to increase awareness of how to construct reality and to break free of limiting structures that shape our understanding.4
In a recent article posted on The Edvocate website entitled Teaching Social Justice in Your Classroom, Mathew Lynch provides some activities that can be used to develop the skills necessary to advance social justice.3
These skills include:
· Differentiating between fact and opinion to determine what is true
· Examining diverse points of view to look at an issue from all sides
· Developing a personal perspective based on accurate comprehension
Given that the majority of health professions students come from diverse backgrounds, these skills are not only relevant when treating patients, but also when interacting and working with classmates. Even more reason to explore social justice! Students should be able to have a healthy dialogue with persons of different ethnicities, gender, age, and religious beliefs.
In a recent article posted on the Resilient Educator website entitled Teaching Social Justice in Theory and Practice by Caitrin Blake, the author suggests using these questions to explore potential systemic inequality in public policy … or healthcare delivery:1
· Who makes decisions and who is left out?
· Who benefits and who suffers?
· Why is a given practice fair or unfair?
· What is required to create change?
· What alternatives can we imagine?
Blake suggests, in order to foster social justice in the classroom, educators must first build a safe, encouraging place where students can speak about their experiences and beliefs.1 Thought-provoking conversations can be created by encouraging students to share their ideas and respectfully respond to others without shutting the discussion down.
Social justice cannot be taught and fully understood overnight. Starting the dialogue in the classroom affords students the opportunity to engage in an authentic examination of their world and to work toward positive changes that make healthcare delivery more equitable. Providing a safe environment for students to share personal stories and opinions on different aspects of social justice is just the start. Consider how you might discuss social justice topics with your colleagues and introduce these concepts to your students.
References
- Blake C. Teaching social justice in theory and practice. Resilient Educator [Internet]. 2015 May 13. Available from https://education.cu-portland.edu/blog/classroom-resources/teaching-social-justice/
- Germain D St. Practical Strategy for Infusing Multicultural Content into Any Lesson. Faculty Focus [Internet]. 2019 Nov 11. Available from: https://www.facultyfocus.com/articles/effective-teaching-strategies/infusing-multicultural-content-into-any-lesson/
- Lynch M. Teaching Social Justice in Your Classroom. The Edvocate [Internet]. 2019 Jan 9. Available from: https://www.theedadvocate.org/teaching-social-justice-in-your-classroom/
- Sukhera J, Watling CJ, Gonzalez CM. Implicit Bias in Health Professions: From Recognition to Transformation. Acad Med. 2020;95:717‐723.
- Van Ryn M, Hardeman R, Phelan SM, et al. Medical school experiences associated with change in implicit racial bias among 3547 students: A medical student CHANGES study report. J Gen Intern Med. 2015; 30:17



